The following are from Research Papers and Scientific publication.
To read the actual papers go to the links.
Morgellons disease, illuminating an undefined illness:
a case series
by William T. Harvey, Robert C. Bransfield, Dana E. Mercer,
Andrew J. Wright, Rebecca M. Ricchi and Mary M Leitao
http://www.biomedcentral.com/content/pdf/1752-1947-0003-0000008243.pdf
Proposed Characterization of Morgellons Disease
Morgellons disease is a multi-systemic illness manifests as a skin phenomenon, an immune deficiency state and a chronic inflammatory process. Since infectious agents can initiate and maintain chronic diseases, the behavioral and other CNS manifestations here are more likely effect than cause. Morgellons is a chronic infectious process.
The most common physical abnormalities (symptoms) found in this series (research) include:
1) Numerous “senile angiomas” on the trunk, head and limbs of many;
2) Recurrent fever;
3) Awareness of itching, crawling, stinging or biting. When present, patients describe a circadian tempo to the symptoms; some occurring solely at night. Itching of unbroken skin specifically appeared to precede all other skin symptoms;
4) Unidentified objects (called “filaments” or “granules”) “extrude” uncomfortably from unbroken skin or skin lesions;
5) Painful ulcer-like concave, circular skin lesions with distinct border;
6) Excoriations adjacentto but separate from ulcerations were common;
7) Dermal symptoms were the central focus of discomfort for most patients.
8. Multiple organ system symptoms often appeared within the first six months of illness onset. The most common systems affected were the central and peripheral nervous systems, autonomic nervous system then endocrine, cardiovascular, and pulmonary systems
Primary Abnormal Findings
1. The large age spread, geographic spread and gender neutrality among patients suggest broad human susceptibility to the illness.
2. Rural abode or exposure to unhygienic conditions (third world travel or simply soil exposure) may be risk factors.
3. Onset rate is moderately rapid, without recognizable prodrome, commonly preceded by a healthy state.
4. Once ill, exercise capacity is significantly reduced.
5. The illness is common among family members and close associates, both related genetically and unrelated (such as spouses).
6. Most patients experience weight gain after disease onset.
7. Micro-angiomas appear rapidly on skin after illness onset in most.
8. Fever is recurrent in at least half of those affected.
9. The first illness sign may be the sudden appearance of persistent itching. Ulcerative lesions follow in some cases.
10. Once dermal symptoms begin, patients experience extrusion of unfamiliar material described variously as filamentous, “fuzz balls”, black or white “flecks” or “rice grains”.
11. Numerous CNS effects occur, that includes bizarre cranial nerve phenomena, anxiety and emotional sequelae. The former tend to be transient.
12. Numerous Peripheral Nervous System findings appear after illness onset. Unlike CNS effects, these are serious, permanent and progressive, and include sensory and motor nerves.
13. All Morgellons have elevated heart rate (>72 BPM) and low body temperature by oral thermometry (<97.5 degrees F).
14. Orthostatic intolerance is intermittent but common in most.
15. Most have some formally diagnosable emotional illness that begins with or becomes apparent after Morgellons disease onset.
16. Endocrine abnormality number and type is higher than background. Most common are Diabetes Type II, Hashimoto’s Thyroiditis, hyperparathyroidism and adrenal hypofunction.
17. Most have elevated fasting insulin levels accompanied by elevated TNF-alpha (insulin receptor blocker)
Basic Background Data
Demographics
Countries of origin: U.S., U.K., Canada, Japan
Male:Female ratio approximates 50:50
Age range: 10-75 years
24/25 were Caucasian
Urban: Rural ratio = 50:50
Past medical history
11out of 25 were diagnosed with bipolar disease
7 out of 25 were diagnosed with adult ADD
1 out of 25 was diagnosed with schizophrenia
Common childhood illnesses were absent regardless of vaccination status
19 out of 25 had been given general anesthesia at least once
9 out of 25 had prior orthopedic surgery
6 out of 25 had other prior surgery for chronic inflammatory diseases (appendix, gallbladder)
Illness History
Time from initiation to full onset: several months
Exposure to unhygienic conditions occurred several days to several weeks prior to illness onset Patients claimed relative healthiness prior to Morgellons (as initially described) onset; No consistent recognized prodrome heralded onset of the illness Allergy symptoms were rare Activating stressor event was present in 1 out of 3 of cases
Social History
50% were married/ 50% single
28% were smokers
None routinely exercised
Dermatologic
24% of patients had dark filaments visibly protruding from the skin 17 out of 25 had frequent skin eruptions/rashes Just over 50% experienced no movement sensations
Only 50% itched regularly
72% has angiomata appear
Central Nervous System
Over half had frequent headaches
Over half had unstable visual acuity including double vision (10 out of 25)
10 out of 25 reported visual “flashes” (not characterized) in either daylight or dark
Emotional liability in half of patients 1/3 reported frequent dizziness
1/3 reported permanent hearing loss (degree not determined)
40% reported tinnitus
20 out of 25 reported frequent occurrence of forgetfulness
12 out of 25 had persistent regional skin numbness
6 out of 25 had persistent tremors
Metabolic
Average weight gain after onset: 33 lbs
20 out of 25 experienced regular high levels of fatigue
25% were intolerant to cold and 25% intolerant to heat (some overlap, but degree undetermined)
10 out of 25 reported sweating inappropriately (either under- or over-sweating)
Immune
12 out of 25 had cyclical fever
18 out of 25 reported numerous angiomas verified by examination
10 out of 25 reported many “colds” annually
8 out of 25 reported “chronic sinusitis”
4 out of 25 reported frequent sore throats over a period of years
2 out of 25 reported frequent toothaches
Endocrine
8 out of 25 had prior diagnosis of Hashimoto’s Thyroiditis
50% had hypercalcemia, 3 of whom had parathyroid adenomas
Fasting insulin levels were elevated in all tested (6 out of 25)
Corticotrophin Releasing Hormone (CRH) levels were elevated in all tested
Musculo-skeletal
15 out of 25 reported frequent neck pain
10 out of 25 had persistent limited neck movement
22 out of 25 had chronic musculoskeletal pain, without arthritis
Pain was constant and incapacitating in 1/3 of patients
Gastro-intestinal
50% had constipation or diarrhea, or both (overlap was common)
25% had chronic nausea
Pulmonary
Persistent cough (non-productive, non-wheezing) in 9 out of 25†
Persistent dyspnea in 7 out of 25
Emotional
Half reported “anxiety”
Half reported frequent mood swings
Half reported frequent depression
Other
Urine stream control problems in 6 out of 25
1 Less than half of the 25 patients studied reported the presence of filaments, and as a result, the authors did not search for filaments on all patients.
2 Average weight gain in male and female patients combined. Time period for weight gain undetermined.
Vital Signs
Average temp 97.51° F
Average pulse 85.32 BPM
Laboratory Data
Unidentified lymphatic filamentous clusters were found in 4 patients
50% were positive for Borrelia burgdorferi sensu lato either by CDC Western
Blot (WB) criteria, EUCALB WB (IgM P31 and 34 added), or IFA
4 patients were seropositive for Babesia microti
92% were seropositive for Chlamydia pneumonia (Chp)
1 Suggests Borrelia may contribute to some cases of Morgellons disease.
2 Suggests Babesia is uncommon in most Morgellons disease cases.
3 Suggests Chlamydia pneumonia (Chp) is one candidate for the initial etiology of Morgellons disease via generation of an immunodeficiency state.
4 Lab tests were drawn at 6,100 feet MSL (above mean sea level).
5 RBC characteristics were adjusted for elevation. All indices should be “normal.”
6 Lower than regional mean of 66%.
7 Slightly higher than regional mean of 28%.
8 Much higher than regional mean of 3.0%.
9 Although a broad “normal” range exists for NK number, our clinical experience supports that consistently healthy individuals who rarely experience viral
syndromes have NK # > 200. Our patients’ range is not infrequently below 10. This suggests one component of an immune deficiency state.
10 Well above regional mean of 84.
11 Well above regional mean of 0.6.
12 Although clearly “within range” at 6,100 ft. MSL, the mean of more than 100 similar patients tested near sea level (2001-2004) was 18 (21-28 anticipated).
As low CO2 level translates to low serum bicarbonate level, this suggests required buffering to lower acidity. Although there are several causes of elevated serum acidity, many of these patients underwent overnight studies for sleep apnea that revealed consistent low breathing rate raising PCO2. No such formal test was included in testing these patients although we believe such testing would be highly revealing.
13 Despite this average being satisfactory, 7 of the 25 patients tested were between 10.0 and 10.6. Three of 25 patients were found to have parathyroid adenomas.
14Greater than 5.0 in 9 of 25.
15 The converse of immune deficiency, however, suggests that a possible chronic infectious state may have been operant that could intermittently activate humoral immunity.
16 Commonly above 2.0. As globulin is elevated and albumin is clearly not low, the ratio elevation is driven somehow by the albumin. This is presently a paradox.
17 Average is high normal and well above the regional mean of 68. Suggests skeletal involvement in the disease, although liver involvement is possible. Most Morgellons patients have shown evidence of osteopenia or osteoporosis when randomly tested despite age. Bone density was not determined in these 25 patients. We believe doing so would be valuable.
18 Argues against an autoimmune role, particularly as 5 out of 25 were 0, and all were less than 20.
19 Despite this normal finding, Hashimoto’s Thyroiditis is common in larger similar groups of Morgellons. Further evaluation of the HP axis and the endocrine system in general should be included in any future studies.
20 Currently used to assess cardiac risk in three stages. In this context, we are assessing chronic inflammation. This average supports the presence of a persistent inflammatory process that parallels physical evidence of vasculitis.
21 Five >150, suggests cytokine activation and possible inflammatory effect.
22 High-normal. 11 out of 25 >3.6, suggests cytokine activation and possible inflammatory effect.
23 Definite elevation in 92%. Most commonly corresponds to insulin receptor blockade and to chronic inflammatory effects.
24 Elevation of Transforming Growth Factor beta (TGF-beta) can occur when pathological events diminish its protective growth modulating effects on various tissues. This test result parallels evidence of excessive growth processes observed in these patients such as numerous angiomata, skin tags, nevi, and regions of increased epidermis density.
25 Consistently elevated in most male and female study patients. Parallels the gain in body fat and angiogenesis experienced by most following illness onset.
SEPARATE FROM THE ABOVE FROM
Recovery of Morgellons-Related Particles From Water Samples
October 9, 2012http://www.morgellons-uk.net/?p=850
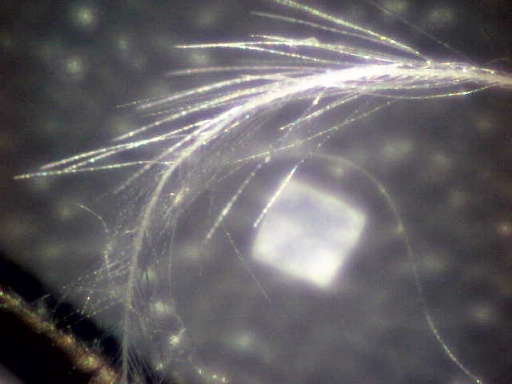
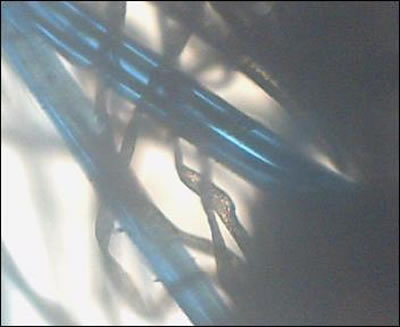
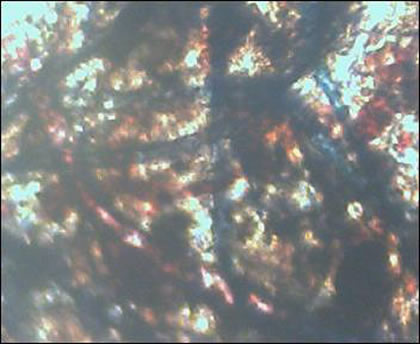
In this article scientists found Morgellons fibers living in a hot water heater causing chronic skin irritation and other deblilitating symptoms to the scalp, neck and shoulders of the homeowner. The hot water tank had been idle for more than 2 years and is thought to have been contaminated by soil/groundwater organisms. Replacement of the hot water system and water pipes eliminated these contaminants and resulted in a marked improvement in the homeowner’s health. Microscopic examination and microbial analysis of water samples collected before hot tank removal show the presence of numerous fiber-producing microorganisms.
Agrobacterium & Morgellons Disease, A GM Connection?
April 29, 2008 http://www.morgellons-uk.net/?p=413
In other words, Agrobacterium persisting in transgenic plants released into the environment has the potential to spread new diseases, and to plants that normally would not be infected by the disease agents. At the time, the researchers did not know that Agrobacterium would also infect animals and humans, and could spread new diseases to them as well.
Have these warnings been heeded by other researchers? There is no evidence they have been taken on board. Agrobacterium has since been shown to transform at least 80 different non-plant species including yeasts and other fungi, algae, mammalian and human cells, also the gram positive bacterium Streptomyces lividans. In a recent review, the researchers stated: “Future research has to show whether Agrobacterium-mediated transformation contributed to horizontal gene transfer between microorganisms in the rhizosphere.”
GOING AWAY
IMAGINED
A PARASITE
FIBERS FROM CLOTHING SCRATCHED INTO THE SKIN
To read the actual papers go to the links.
Morgellons disease, illuminating an undefined illness:
a case series
by William T. Harvey, Robert C. Bransfield, Dana E. Mercer,
Andrew J. Wright, Rebecca M. Ricchi and Mary M Leitao
http://www.biomedcentral.com/content/pdf/1752-1947-0003-0000008243.pdf
Proposed Characterization of Morgellons Disease
Morgellons disease is a multi-systemic illness manifests as a skin phenomenon, an immune deficiency state and a chronic inflammatory process. Since infectious agents can initiate and maintain chronic diseases, the behavioral and other CNS manifestations here are more likely effect than cause. Morgellons is a chronic infectious process.
The most common physical abnormalities (symptoms) found in this series (research) include:
1) Numerous “senile angiomas” on the trunk, head and limbs of many;
2) Recurrent fever;
3) Awareness of itching, crawling, stinging or biting. When present, patients describe a circadian tempo to the symptoms; some occurring solely at night. Itching of unbroken skin specifically appeared to precede all other skin symptoms;
4) Unidentified objects (called “filaments” or “granules”) “extrude” uncomfortably from unbroken skin or skin lesions;
5) Painful ulcer-like concave, circular skin lesions with distinct border;
6) Excoriations adjacentto but separate from ulcerations were common;
7) Dermal symptoms were the central focus of discomfort for most patients.
8. Multiple organ system symptoms often appeared within the first six months of illness onset. The most common systems affected were the central and peripheral nervous systems, autonomic nervous system then endocrine, cardiovascular, and pulmonary systems
Primary Abnormal Findings
1. The large age spread, geographic spread and gender neutrality among patients suggest broad human susceptibility to the illness.
2. Rural abode or exposure to unhygienic conditions (third world travel or simply soil exposure) may be risk factors.
3. Onset rate is moderately rapid, without recognizable prodrome, commonly preceded by a healthy state.
4. Once ill, exercise capacity is significantly reduced.
5. The illness is common among family members and close associates, both related genetically and unrelated (such as spouses).
6. Most patients experience weight gain after disease onset.
7. Micro-angiomas appear rapidly on skin after illness onset in most.
8. Fever is recurrent in at least half of those affected.
9. The first illness sign may be the sudden appearance of persistent itching. Ulcerative lesions follow in some cases.
10. Once dermal symptoms begin, patients experience extrusion of unfamiliar material described variously as filamentous, “fuzz balls”, black or white “flecks” or “rice grains”.
11. Numerous CNS effects occur, that includes bizarre cranial nerve phenomena, anxiety and emotional sequelae. The former tend to be transient.
12. Numerous Peripheral Nervous System findings appear after illness onset. Unlike CNS effects, these are serious, permanent and progressive, and include sensory and motor nerves.
13. All Morgellons have elevated heart rate (>72 BPM) and low body temperature by oral thermometry (<97.5 degrees F).
14. Orthostatic intolerance is intermittent but common in most.
15. Most have some formally diagnosable emotional illness that begins with or becomes apparent after Morgellons disease onset.
16. Endocrine abnormality number and type is higher than background. Most common are Diabetes Type II, Hashimoto’s Thyroiditis, hyperparathyroidism and adrenal hypofunction.
17. Most have elevated fasting insulin levels accompanied by elevated TNF-alpha (insulin receptor blocker)
Basic Background Data
Demographics
Countries of origin: U.S., U.K., Canada, Japan
Male:Female ratio approximates 50:50
Age range: 10-75 years
24/25 were Caucasian
Urban: Rural ratio = 50:50
Past medical history
11out of 25 were diagnosed with bipolar disease
7 out of 25 were diagnosed with adult ADD
1 out of 25 was diagnosed with schizophrenia
Common childhood illnesses were absent regardless of vaccination status
19 out of 25 had been given general anesthesia at least once
9 out of 25 had prior orthopedic surgery
6 out of 25 had other prior surgery for chronic inflammatory diseases (appendix, gallbladder)
Illness History
Time from initiation to full onset: several months
Exposure to unhygienic conditions occurred several days to several weeks prior to illness onset Patients claimed relative healthiness prior to Morgellons (as initially described) onset; No consistent recognized prodrome heralded onset of the illness Allergy symptoms were rare Activating stressor event was present in 1 out of 3 of cases
Social History
50% were married/ 50% single
28% were smokers
None routinely exercised
Dermatologic
24% of patients had dark filaments visibly protruding from the skin 17 out of 25 had frequent skin eruptions/rashes Just over 50% experienced no movement sensations
Only 50% itched regularly
72% has angiomata appear
Central Nervous System
Over half had frequent headaches
Over half had unstable visual acuity including double vision (10 out of 25)
10 out of 25 reported visual “flashes” (not characterized) in either daylight or dark
Emotional liability in half of patients 1/3 reported frequent dizziness
1/3 reported permanent hearing loss (degree not determined)
40% reported tinnitus
20 out of 25 reported frequent occurrence of forgetfulness
12 out of 25 had persistent regional skin numbness
6 out of 25 had persistent tremors
Metabolic
Average weight gain after onset: 33 lbs
20 out of 25 experienced regular high levels of fatigue
25% were intolerant to cold and 25% intolerant to heat (some overlap, but degree undetermined)
10 out of 25 reported sweating inappropriately (either under- or over-sweating)
Immune
12 out of 25 had cyclical fever
18 out of 25 reported numerous angiomas verified by examination
10 out of 25 reported many “colds” annually
8 out of 25 reported “chronic sinusitis”
4 out of 25 reported frequent sore throats over a period of years
2 out of 25 reported frequent toothaches
Endocrine
8 out of 25 had prior diagnosis of Hashimoto’s Thyroiditis
50% had hypercalcemia, 3 of whom had parathyroid adenomas
Fasting insulin levels were elevated in all tested (6 out of 25)
Corticotrophin Releasing Hormone (CRH) levels were elevated in all tested
Musculo-skeletal
15 out of 25 reported frequent neck pain
10 out of 25 had persistent limited neck movement
22 out of 25 had chronic musculoskeletal pain, without arthritis
Pain was constant and incapacitating in 1/3 of patients
Gastro-intestinal
50% had constipation or diarrhea, or both (overlap was common)
25% had chronic nausea
Pulmonary
Persistent cough (non-productive, non-wheezing) in 9 out of 25†
Persistent dyspnea in 7 out of 25
Emotional
Half reported “anxiety”
Half reported frequent mood swings
Half reported frequent depression
Other
Urine stream control problems in 6 out of 25
1 Less than half of the 25 patients studied reported the presence of filaments, and as a result, the authors did not search for filaments on all patients.
2 Average weight gain in male and female patients combined. Time period for weight gain undetermined.
Vital Signs
Average temp 97.51° F
Average pulse 85.32 BPM
Laboratory Data
Unidentified lymphatic filamentous clusters were found in 4 patients
50% were positive for Borrelia burgdorferi sensu lato either by CDC Western
Blot (WB) criteria, EUCALB WB (IgM P31 and 34 added), or IFA
4 patients were seropositive for Babesia microti
92% were seropositive for Chlamydia pneumonia (Chp)
1 Suggests Borrelia may contribute to some cases of Morgellons disease.
2 Suggests Babesia is uncommon in most Morgellons disease cases.
3 Suggests Chlamydia pneumonia (Chp) is one candidate for the initial etiology of Morgellons disease via generation of an immunodeficiency state.
4 Lab tests were drawn at 6,100 feet MSL (above mean sea level).
5 RBC characteristics were adjusted for elevation. All indices should be “normal.”
6 Lower than regional mean of 66%.
7 Slightly higher than regional mean of 28%.
8 Much higher than regional mean of 3.0%.
9 Although a broad “normal” range exists for NK number, our clinical experience supports that consistently healthy individuals who rarely experience viral
syndromes have NK # > 200. Our patients’ range is not infrequently below 10. This suggests one component of an immune deficiency state.
10 Well above regional mean of 84.
11 Well above regional mean of 0.6.
12 Although clearly “within range” at 6,100 ft. MSL, the mean of more than 100 similar patients tested near sea level (2001-2004) was 18 (21-28 anticipated).
As low CO2 level translates to low serum bicarbonate level, this suggests required buffering to lower acidity. Although there are several causes of elevated serum acidity, many of these patients underwent overnight studies for sleep apnea that revealed consistent low breathing rate raising PCO2. No such formal test was included in testing these patients although we believe such testing would be highly revealing.
13 Despite this average being satisfactory, 7 of the 25 patients tested were between 10.0 and 10.6. Three of 25 patients were found to have parathyroid adenomas.
14Greater than 5.0 in 9 of 25.
15 The converse of immune deficiency, however, suggests that a possible chronic infectious state may have been operant that could intermittently activate humoral immunity.
16 Commonly above 2.0. As globulin is elevated and albumin is clearly not low, the ratio elevation is driven somehow by the albumin. This is presently a paradox.
17 Average is high normal and well above the regional mean of 68. Suggests skeletal involvement in the disease, although liver involvement is possible. Most Morgellons patients have shown evidence of osteopenia or osteoporosis when randomly tested despite age. Bone density was not determined in these 25 patients. We believe doing so would be valuable.
18 Argues against an autoimmune role, particularly as 5 out of 25 were 0, and all were less than 20.
19 Despite this normal finding, Hashimoto’s Thyroiditis is common in larger similar groups of Morgellons. Further evaluation of the HP axis and the endocrine system in general should be included in any future studies.
20 Currently used to assess cardiac risk in three stages. In this context, we are assessing chronic inflammation. This average supports the presence of a persistent inflammatory process that parallels physical evidence of vasculitis.
21 Five >150, suggests cytokine activation and possible inflammatory effect.
22 High-normal. 11 out of 25 >3.6, suggests cytokine activation and possible inflammatory effect.
23 Definite elevation in 92%. Most commonly corresponds to insulin receptor blockade and to chronic inflammatory effects.
24 Elevation of Transforming Growth Factor beta (TGF-beta) can occur when pathological events diminish its protective growth modulating effects on various tissues. This test result parallels evidence of excessive growth processes observed in these patients such as numerous angiomata, skin tags, nevi, and regions of increased epidermis density.
25 Consistently elevated in most male and female study patients. Parallels the gain in body fat and angiogenesis experienced by most following illness onset.
SEPARATE FROM THE ABOVE FROM
Recovery of Morgellons-Related Particles From Water Samples
October 9, 2012http://www.morgellons-uk.net/?p=850
In this article scientists found Morgellons fibers living in a hot water heater causing chronic skin irritation and other deblilitating symptoms to the scalp, neck and shoulders of the homeowner. The hot water tank had been idle for more than 2 years and is thought to have been contaminated by soil/groundwater organisms. Replacement of the hot water system and water pipes eliminated these contaminants and resulted in a marked improvement in the homeowner’s health. Microscopic examination and microbial analysis of water samples collected before hot tank removal show the presence of numerous fiber-producing microorganisms.
Agrobacterium & Morgellons Disease, A GM Connection?
April 29, 2008 http://www.morgellons-uk.net/?p=413
In other words, Agrobacterium persisting in transgenic plants released into the environment has the potential to spread new diseases, and to plants that normally would not be infected by the disease agents. At the time, the researchers did not know that Agrobacterium would also infect animals and humans, and could spread new diseases to them as well.
Have these warnings been heeded by other researchers? There is no evidence they have been taken on board. Agrobacterium has since been shown to transform at least 80 different non-plant species including yeasts and other fungi, algae, mammalian and human cells, also the gram positive bacterium Streptomyces lividans. In a recent review, the researchers stated: “Future research has to show whether Agrobacterium-mediated transformation contributed to horizontal gene transfer between microorganisms in the rhizosphere.”
GOING AWAY
IMAGINED
A PARASITE
FIBERS FROM CLOTHING SCRATCHED INTO THE SKIN

IS
IS NOT



Morgellons is showing up in allanimals:
humans, dogs, cats, elephants, horses, cows, frogs, lizards, and bugs, bees, wasps ....
It lives in the air, water, dirt, inside animals, insects and us.
It is global.
Currently the only suggestion I have is to get healthy. All of those afflicted had weak
immune systems.
Eat real organic food. Bath. Clean your home.
humans, dogs, cats, elephants, horses, cows, frogs, lizards, and bugs, bees, wasps ....
It lives in the air, water, dirt, inside animals, insects and us.
It is global.
Currently the only suggestion I have is to get healthy. All of those afflicted had weak
immune systems.
Eat real organic food. Bath. Clean your home.